Last week, a new retrospective study from Tongji Hospital in Wuhan was published in Science China Life Sciences (a Springer Link journal). The study found 47% fatalities in critically ill #COVID19 patients that were given regular treatment, and only 19% fatalities in patients treated with low doses of hydroxychloroquine (HCQ).
These results sound amazing.
But I took a closer look. And I have lots of questions.
The paper

Here is the paper: Low dose of hydroxychloroquine reduces fatality of critically ill patients with COVID-19 – Bo Yu et al., Science China Life Sciences (2020), DOI: 10.1007/s11427-020-1732-2.
In the paper, Yu et al describe a group of 550 critically ill COVID-19 patients , 48 of whom were treated with a low dose of oral HCQ treatment (200 mg twice a day). They report 19% fatalities in the HCQ group and 47% in the non-HCQ group.
Most of my comments here were also posted on PubPeer and in a Twitter thread.
The paper had been published earlier as a preprint on MedRxiv, and critically discussed in a Twitter thread by Dr. Gaetan Burgio on May 2, 2020. The main difference between the preprint and this paper appears to be that 18 controls were taken out of the study and 5 authors were added.
Grant support: “This work was supported in part by projects from Ministry of Science and Technology of China (2020YFC0844500), the National Natural Science Foundation of China (31130031), Emergency Project Fund of Chinese Academy of Sciences (2020YJFK0105) and Chinese Academy of Engineering and Ma Yun Foundation (2020-CMKYGG-05).“
Concerns about ethical approval
The Methods state “This study has been approved by the institutional review board of Tongji Hospital (IRBID: TJ-C20200113). The written informed consent has been waived by the Ethics Committee because of the retrospective and anonymous nature of the data.“
Although patient data reported in the paper appears to be indeed anonymous, consent might still need to be applicable since the patients received a treatment that is experimental and not standard-of-care. It is not sure if patients or their family agree to be treated with HCQ. This might not be a problem, however, depending on local rules. Maybe there was a general consensus that HCQ did not need patient’s consent to be administered.
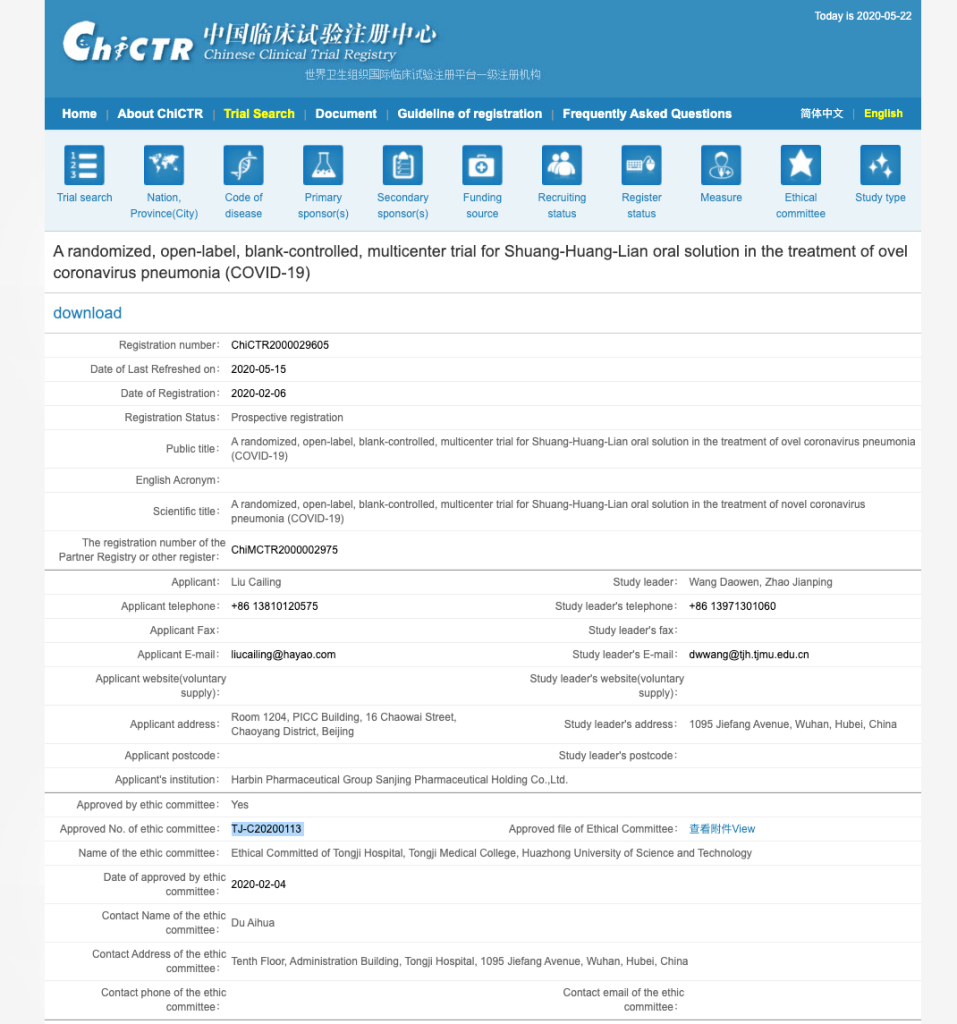
Another concern was pointed out to me by two Twitter users. On the Chinese Clinical Trial Registry website, the IRB number listed above (TJ-C20200113) is assigned to a different study, i.e. a randomized prospective multicenter trial of Shuang-Huang-Lian oral solution as a treatment of COVID-19 cases, led by the same senior author as this HCQ study. The Shuang-Huang-Lian study was approved on February 4, three days after the HCQ study started.
According an article in Korea Biomedical Review, Shuang-Huang-Lian is a mixture of honeysuckle flowers, Chinese skullcap, and forsythia. This traditional Chinese medicine (TCM) mixture was promoted as very effective for treating COVID-19, but was called “Snake Oil” by the Foreign Policy.
Forsythia, coincidentally, also is the name of the homeopathic snake oil in the movie Contagion. But I digress.
So the IRB approval number obtained for a prospective, randomized study on a flower mixture appears to be reused to cover a retrospective, unrandomized study on hydroxychloroquine. That appears to be unethical. These are two unrelated studies, and approval to conduct one study cannot be transferred to another study involving a different drug.
Number anomalies in Table 1
Table 1 gives a bunch of baseline characteristics that appear to contain some inconsistencies.
- Under Symptoms the majority of the patients (77%) is listed as having a fever at baseline (marked below in blue). However, under vital signs the median body temp is listed as 36.6 °C (Q1-Q3 range 36.3-37.0). That does not appear to be very feverish to me.
- Under Symptoms data is only given for 458 patients. Does that mean that for almost 100 patients the data was not available? How about the other categories, such as Vital Signs and Laboratory Parameters? Is that data given for all 550 patients or only for 458? Body temp, pulse, etc are not fancy measurements. It is of concern that 17% of data was not available.
- Under Vital signs, the medians of All Patients appear to not match those of the two subgroups. These values are highlighted below in red. For example, the median blood pressure in the combined group is 130, but in the two subgroups it is 131 and 133. This is not mathematically possible. As @NeuroOscillator pointed out on Twitter “A pooled median is guaranteed to be between the subgroup medians”. Except in this paper.

4. Another strange anomaly is Table 1 (at the bottom) states that only 63.5% of the patients were on mechanical ventilation. The abstract states “we included 550 critically ill COVID-19 patients who need mechanical ventilation” – suggesting that all of them were on ventilation. It is also worth pointing out that the percentage of ventilated patients was higher in the NHCQ group (63.9% vs. 58.3% in the HCQ group) although that this was not statistically significant.
The month that had 60 days
Most of us would agree that the month of April felt like the longest month ever. Working from home during a shelter in place, no commute, not seeing friends or going out, with kids at home, endless zoom meetings, maybe loss of jobs or financial worries, illness and death, horrible news all over the world …. the month did not seem to end.
Well, it looks like we were not wrong. According to the Yu paper, April 2020 might indeed have had at least 60 days.
The Results has the following wording: “From February 1, 2020 to April 4, 2020, a total of 550 critically ill COVID-19 patients were admitted to Tongji Hospital, including 344 males and 206 females.“
So let’s look at the time intervals and see if they match:
- Patients were admitted until as late as April 4
- Figure 1 shows the patient survival up to 60 days since admission.
- Table 3 gives the fatality risks at 60 days post HCQ treatment.
- The paper was submitted to the journal on April 23, 2020.

Somehow I have trouble fitting a 60-day interval between April 4 (last patient admission) and April 23 (paper submission).
With a paper submission date of April 23, a 60 day time span should have started on February 23 according to my calculations.
Did April indeed have 60 days, or is something else off?


The paper was previously published as preprint:
https://www.medrxiv.org/content/10.1101/2020.04.27.20073379v1
Didier Raoult was very excited:
Swiftly debunked by Gaetan Burgio:
More here:
https://forbetterscience.com/2020/04/22/chloroquine-witchdoctor-didier-raoult-barking-mad-and-dangerous/
LikeLike
Lancet to review reliability of data.
https://www.theguardian.com/world/2020/jun/03/covid-19-surgisphere-who-world-health-organization-hydroxychloroquine
Governments and WHO changed Covid-19 policy based on suspect data from tiny US company
Surgisphere, whose employees appear to include a sci-fi writer and adult content model, provided database behind Lancet and New England Journal of Medicine hydroxychloroquine studies.
“Lancet editor Richard Horton told the Guardian: “Given the questions raised about the reliability of the data gathered by Surgisphere, we have today issued an Expression of Concern, pending further investigation.
“An independent data audit is currently underway and we trust that this review, which should be completed within the next week, will tell us more about the status of the findings reported in the paper by Mandeep Mehra and colleagues.”
LikeLike